3. Structure of PROMS. What outcomes are important?
Patient-reported outcomes (PROs) must be carefully defined to ensure they capture aspects of health that matter to patients. Equally important, these outcomes should be measured accurately and—where possible—in ways that are comparable across settings.
Before exploring PROs in more depth, it is helpful to understand the following key definitions:
Patient-reported outcome measures (PROMs) are standardised, validated questionnaires (also called instruments, scales or tools), plus the documentation that supports their use, completed by patients to capture their perception of functional well-being and health status.
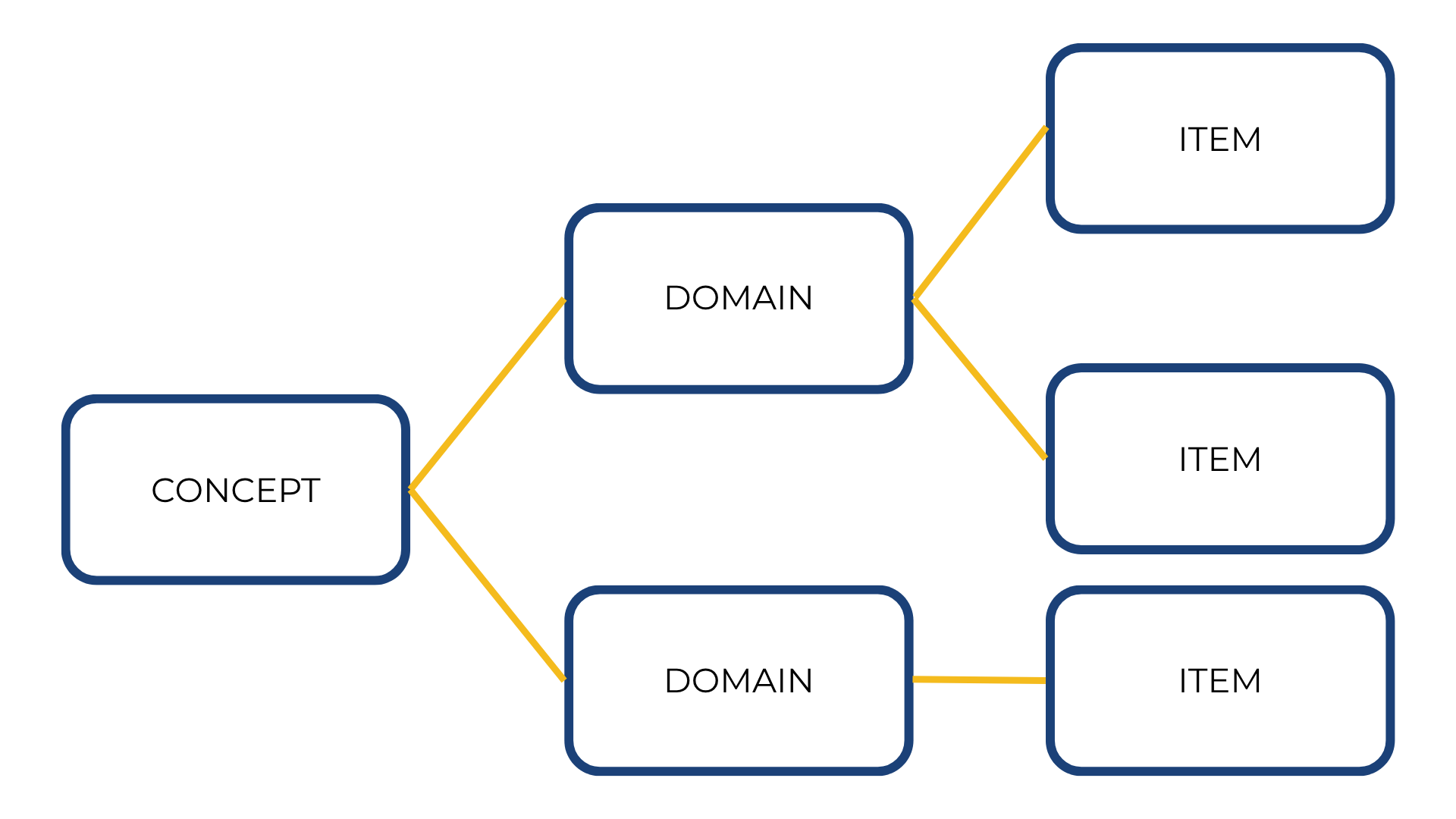
A sub-concept represented by a score of a PROM that measures a larger concept composed of multiple domains.
Example:
Concept = Psychological state → Domain = Depression
An individual question, statement, or task (and its standardised response options) that is evaluated by the patient to address a particular concept.
Example:
Concept = Psychological state → Domain = Depression → Item = “Are you feeling depressed?”
The conceptual framework explicitly defines the concepts measured by the instrument in a diagram that presents a description of the relationships between items, domain (sub-concepts) and concepts measured and the scores produced by a PRO instrument (Figure 1 )
Importance of Clear and Specific Items
The way questions (items) are formulated matters greatly – Vague items (for example ‘How are you feeling on a scale of 1 to 10?’ where 1 is poorly and 10 being extremely well) provide little useful information. More specific questions relating to emotional wellbeing (concept) influenced by mobility, ease of breathing, etc. (domains), will provide more detailed and specific information.
Deciding what to measure and how specific to be is therefore critical. It is important to distinguish the concept from the questions that you need to ask to detect and assess a change in the concept.
Example: PROs in Chronic obstructive pulmonary disease (COPD)
For example, investigators researching the response of patients with COPD to a therapy may recognise that these patients may find performing tasks more difficult in the morning. The concept that they decide to measure is the burden and extent of morning symptoms and the ability of patients to perform activities at that time of day.
The items to capture this concept may be questions such as:
- Did you wash yourself this morning other than your face, i.e. body wash, shower, bathe?
- Did you get dressed this morning?
- Did you walk around your home early this morning after taking your medicine?
The optional answers that patients are given to these questions may include a range of responses, such as:
- Yes, I did it myself.
- Yes, but I needed help.
- No, I was unable to.
- No, I did not for other reasons.
Patients may also be given an option to respond to a follow up question, such as ‘How difficult was it for you to perform this task?’
Although some PRO concepts have traditionally been developed by healthcare professionals or caregivers, the role of patients in identifying and shaping these concepts is increasingly recognised.
Table 1 provides an overview of major concepts addressed by PROs. The most commonly used PRO questionnaires assess one of the following constructs:
| Concept | Description |
| 🌍 Quality of Life (QoL) | WHO defines QoL as a person’s perception of their position in life within their cultural and value context. |
| 💗 Health-Related Quality of Life (HRQoL) | Multidimensional evaluation of how health and treatment affect physical, emotional, social, and functional life. |
| 👍 Patient Satisfaction | Evaluation of treatments, preferences, healthcare systems, education, and medical devices. |
| 🏃 Physical Functioning | Physical limitations and restrictions, including mobility, self-care, daily activities, and disability. |
| 🧠 Psychological State | Emotional and cognitive state including anxiety, depression, coping, distress, and well-being. |
| ⚠️ Signs & Symptoms | Reports of symptoms not directly observable, such as fatigue, nausea, or irritability. |
| 🤝 Social Functioning | Restrictions in social activities, work, school, or community participation. |
| 📋 Treatment Adherence | How patients actually follow and use treatments as prescribed. |
| 📊 Utility | A measure of usefulness and patient preferences used in health economics and HTA. |
Table 1: Major concepts measured in PROs