3.1 Calculation and limitations of QALYs
📐 How to Calculate QALYs
QALYs can be calculated using the following formula which assumes a utility value designated by a score (quality of life) between 1 = perfect health and 0 = dead:
This will yield:
- If a person lives in perfect health for one year, that person will have 1 QALY (1 Year of Life × 1 Utility Value = 1 QALY)
- If a person lives in perfect health but only for half a year, that person will have 0.5 QALYs (0.5 Years of Life × 1 Utility Value = 0.5 QALYs)
- Conversely, if a person lives for 1 year in a situation with 0.5 utility (half of perfect health), that person will also have 0.5 QALYs (1 Year of Life × 0.5 Utility Value = 0.5 QALYs)
QALY calculations can be used to visualise the relationship between the quality and quantity of life experienced with and without the therapy in question, as in the graph below.
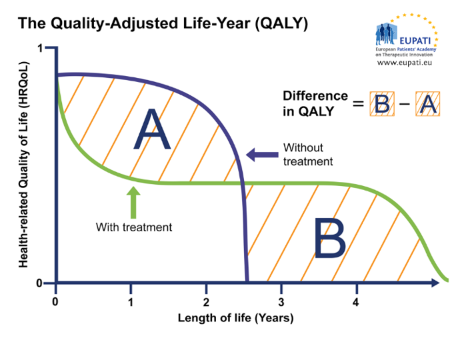
Figure 1: The Quality-Adjusted Life Year (QALY)
Similar graphs can be used to plot changes in HRQoL over time with and without treatment, providing a visualisation of the QALY gain or loss, respectively. In the graph below, for instance, the treatment provides an increase in HRQoL as well as an extension of life, resulting in a net QALY gain.
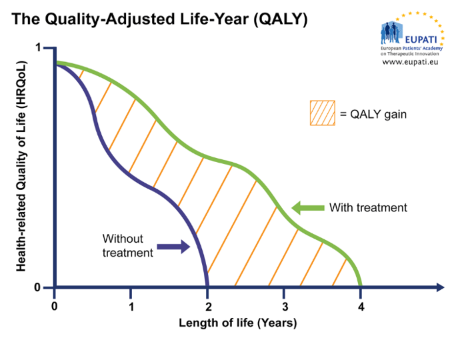
Figure 2: The Quality-Adjusted Life Year (QALY)
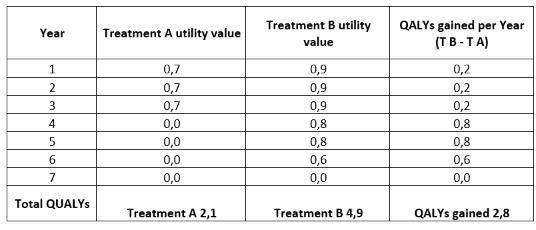
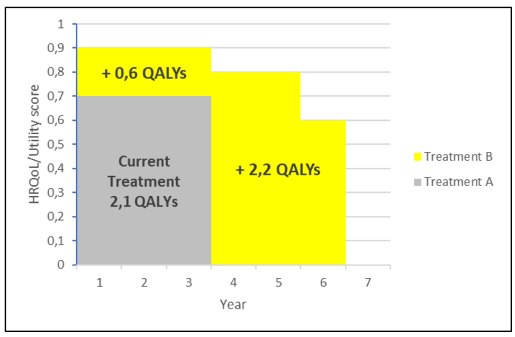
Example: Comparing Two Treatments Using QALYsThe following graph and calculations summarise the essentials of a QALY comparison between two treatments.
|
Limitations of QALY – Critical Debate
The QALY (Quality-Adjusted Life Year) is widely used in health economics to compare medical interventions and allocate healthcare resources. However, the concept remains the subject of critical debate. Discussions typically revolve around three major themes:
A) Ethical Considerations
- Valuing one life over another: The notion of “perfect health” is subjective. Assuming that people with disabilities experience lower quality of life is ethically problematic.
- Reduced patient autonomy: If QALYs are used to justify restricted healthcare budgets or narrow treatment options, this may reduce patients’ freedom to make decisions based on personal needs and values.
- Utilitarian bias: By treating all QALYs as equal, the system implicitly favours maximising total health gains rather than addressing individual or societal priorities. This risks prioritising cost-effectiveness over fairness.
- Equity concerns: QALY-based approaches may systematically disadvantage older individuals, patients with disabilities, or those with chronic conditions, since these groups typically gain fewer QALYs. This also raises concerns about racial and socio-economic disparities, where minority groups may be underrepresented in data or experience comorbidities not fully captured in standard utility values.
A) Methodological and Theoretical Limitations
- Measurement variability:
- Different methods of assessing utility can yield inconsistent results.
- Study participants may misunderstand the utility scales used.
- Diverse populations may value health states differently.
- Contextual factors—severity of initial health state, prevalence of disease, parent or caregiver status, or if a population is marginalised—are often overlooked.
- Definitions of “utility,” its validity, and replicability remain unresolved.
- Mathematical constraints: QALY is calculated as the product of utility and time, where utility is typically scaled between 0 (death) and 1 (perfect health). However, using 0 as a lower bound imposes mathematical limitations, such as preventing division and multiplication involving zero. Some have proposed using consistent units for utility and time to address this.
- Incompatibility across time and populations: Comparing QALYs across different settings (e.g., a 1997 UK study vs. a 2005 German study) may be misleading due to contextual differences, making cross-comparisons potentially flawed.
- Disincentives for innovation: The QALY model assumes constant utility and risk neutrality, which can undervalue new treatments—particularly in fields like regenerative medicine, where initial costs are high but may decrease significantly over time.
- Neglect of rare diseases: Treatments for rare conditions often involve high upfront costs. As QALY evaluations may deem them not cost-effective, this could stifle research and innovation in these areas. In response, countries like the UK have introduced mechanisms such as the Cancer Drugs Fund to fund treatments that may not pass traditional QALY thresholds.
C) Context and Disease-Specific Issues
- Inadequate for some conditions: QALYs may be less meaningful for chronic, non-fatal diseases where improvements in quality of life—not survival—are the primary outcome.
- Life expectancy bias: Since younger, healthier people can potentially gain more QALYs, interventions that benefit the elderly or those with lower life expectancy may be undervalued.
Evidence from ECHOUTCOME
The European Consortium in Healthcare Outcomes and Cost-Benefit Research (ECHOUTCOME) ran a major study on QALYs as used in HTA. They concluded that "preferences expressed by the respondents were not consistent with the QALY theoretical assumptions" that quality of life can be measured in consistent intervals, that life-years and quality of life are independent of each other, that people are neutral about risk, and that willingness to gain or lose life-years is constant over time.[1] .
ECHOUTCOME also released "European Guidelines for Cost-Effectiveness Assessments of Health Technologies," which recommended not using QALYs in healthcare decision making.[2] . Instead, the guidelines recommended that cost-effectiveness analyses focus on "costs per relevant clinical outcome." Instead, the guidelines recommended that cost-effectiveness analyses focus on "costs per relevant clinical outcome."
QALYs have limited value where quality of life is a major consideration but survival is not, thus limiting the utility of the QALY in evaluating the effects of many chronic but not fatal diseases.
In general, younger, healthier groups of people will have many times more QALYs than groups of older, more infirm individuals therefore QALY calculations may undervalue treatments which benefit the elderly or other groups with a lower life expectancy.
📌Interactive activity
Time to test your knowledge: Read the questions carefully and select the correct one. Please note that there is three activities, you can access the different questions using the blue arrows
This is not the assessment, it is just an interactive activity to help you with your learning.
[1] Beresniak, Ariel; Medina-Lara, Antonieta; Auray, Jean Paul; De Wever, Alain; Praet, Jean-Claude; Tarricone, Rosanna; Torbica, Aleksandra; Dupont, Danielle; Lamure, Michel; Duru, Gerard (2015). "Validation of the Underlying Assumptions of the Quality-Adjusted Life-Years Outcome: Results from the ECHOUTCOME European Project". PharmacoEconomics. 33 (1): 61–69. doi:10.1007/s40273-014-0216-0. ISSN 1170-7690. PMID 25230587
[2] European Consortium in Healthcare Outcomes and Cost-Benefit Research (ECHOUTCOME). "European Guidelines for Cost-Effectiveness Assessments of Health Technologies" (PDF). Archived from the original (PDF) on 2015-08-14