The Predictive Value of Non-Clinical Testing
7. Setting the 'First-in-Human' Dose
For many innovative medicines, it is acceptable to estimate the safe start dose for humans. However, for some new medicinal products, an estimate may not be enough to predict serious adverse reactions. Researchers should assess the risk factors and mitigation measures and discuss these before human trials begin. The risk factors should also be taken into account on a medicine by medicine basis.
Risk factors may have to do with the mode of action of the medicine. It is therefore relevant to assess previous human exposure with substances that are related to the medicine, the structure of the medicine, and the evidence from animal models of potential toxicity. Other considerations include nature of the target, intensity effects, and the dose-response relationship. There are risk factors that may require special attention, e.g. metabolic pathways, or inter-species genetic differences . Below are some important factors to consider when the first-in-human dose is set:
- All relevant non-clinical data, including:
- Pharmacological dose response studies;
- Pharmacological/toxicological profile;
- Pharmacokinetics studies.
- The No Observed Adverse Effect Level (NOAEL) is the most important information. NOAEL is the highest dose level that does not produce a significant increase in adverse effects in comparison to the control group. In more simple terms, the NOAEL is the highest dose where no important adverse effects are seen.
- The clinical start dose depends on various factors:
- Pharmacodynamics.
- Particular aspects of the molecule.
- Design of the clinical trials
- Exploratory clinical trials in humans can begin with different, nonclinical support. Therefore, the estimation of the clinical start (and maximal) dose can differ.
Other considerations when setting first-in-human dose are:
If researchers gain early access to human data, it can improve the insight into human physiology/pharmacology. It can also improve the knowledge of a drug’s characteristics and its relevance for the therapeutic target and eventually the disease. The term ‘exploratory clinical trials’ (Phase 0) was developed to meet this need. There are different approaches to carry out such exploratory trials:
- They are to be conducted before or early in Phase I.
- They involve limited human exposure.
- They have no therapeutic intent.
- They are not intended to examine clinical tolerability.
There are two classical ways to establish the first human dose in Phase I (I/II) clinical trials.
-
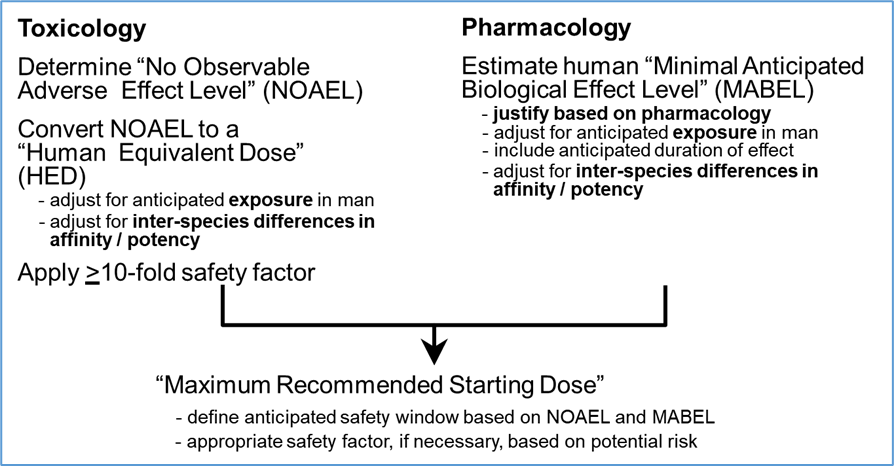
It can be established based on the NOAEL (No Observed Adverse Effect Level) from toxicity studies. A safety factor will have to be taken into consideration as well as individual growth allometric scaling.
- For biologics where their risk factors are identified, it can be established using the Minimal-Anticipated-Biological-Effect-Level (MABEL) standard and also applying a safety factor. To estimate the MABEL, all relevant in vitro and in vivo data are considered. The safety factor is set on the basis of risk criteria. These could for example be how new the active substance is, how potent it is biologically, its mode of action, itsdegree ofspecies specificity, and its dose-response relationship.
The following figure gives a summary of the MABEL approach.
There are other situations, such as clinical trials in cancer patients, where, yet again, other methods may be applied to set the dose.
The Committee for Medicinal Products for Human Use (CHMP) issued a guideline in 2007 on strategies to identify and mitigate risks for first human clinical trials with high risk investigational medicinal products. This guide is recommended to give more information if interested.