Section outline
-
After completing this course, you will be able to:
- Outline the concepts of evidence-based medicine and outcomes research.
EUPATI Open Classroom content is free for all learners.
Enrol & Access the assessment
At the end of each course you can test your knowledge and earn a certificate for a 10-euro administrative fee. If interested, click the button below: -
Evidence-based medicine is a combination of principles and methods. When put into action, these ensure that medical decisions, guidelines and policies are based on the current best evidence about the effects of different forms of treatment and healthcare in general. With respect to medicines, it draws heavily on information from the benefit and risk (efficacy and safety) evaluation.
The concept of evidence-based medicine started in the 1950s. Before then, medical decisions were mainly based on medical training, clinical experience, and journal reading. However, studies showed that medical treatment decisions differed significantly between individual healthcare professionals (Soler & Smith, 2013). The basis was formed for implementing systematic methods to collect, evaluate and organise research data - leading to evidence-based medicine. Since its implementation, evidence-based medicine has been recognised by doctors, pharmaceutical companies, patients, Regulatory Authorities, and the general public.
Evidence-based medicine, as explained by Sackett et al. (1996), includes the conscientious, explicit and judicious use of the best evidence at the current time point. In other words, the evidence must be selected and used carefully, at the right time. Evidence is used to decide how to provide the best possible treatment to a given patient. To do this, the decision maker needs to look at knowledge from their own clinical experience along with the best evidence from controlled studies and research. Combining clinical experience and controlled studies in the decision-making process is important. Without clinical experience, the risk related to a given treatment may end up causing unwanted effects. A decision made with no clinical experience may also be wrong for an individual patient, as the population in a clinical trial might be different from the patient being treated.
The following lessons are about the factors and decisions affecting evidence-based medicine. A common approach to evidence-based medicine is based on a 5 step model:
1. Defining a clinically relevant question
2. Searching for the best evidence.
3. Assessing the quality of the evidence.
4. Acting on the evidence to form a clinical decision.
5. Evaluating the process.Step 1 is relevant in situations where, for example, a patient consults a doctor with a complicated medical problem. The doctor then needs to search for information to find the correct diagnosis. To do so, the doctor needs to define a clinically relevant question. This might include consideration of the population affected (i.e. disease specific), the medical treatment, and the intended outcome.
Having decided upon the clinically relevant question, step 2, a search for the best evidence, must now take place. The person searching for the best evidence needs to be able to critically evaluate the quality of the information found. This is what is meant by step 3, assessing the quality of the evidence. To help with the practical use of evidence-based medicine in daily practice, review databases are available to bring information together. Information that is found can be ranked using the ‘evidence pyramid’ shown in Figure 1.A critical assessment and ranking of the information found is important. The person looking at the information must think about its relevance to the question posed. They must also consider the benefit and risk. Often, generic (non-specific) guidelines and policies exist for whole disease areas, based on the combined evidence. Even though such guidelines are generic, the high degree of evidence is likely to help the decision-making process. Having established the framework, the evidence needs to be used to decide on a particular treatment for the patient, i.e. step 4. After doing so, the choice made needs to be critically evaluated to assess whether the intended outcome was achieved, i.e. step 5.
-
This ranking is particularly relevant if the literature found is inconsistent. The various types of studies listed in Figure 1 will briefly be introduced in the following paragraphs. For further information, refer to the literature listed under ‘further reading’.
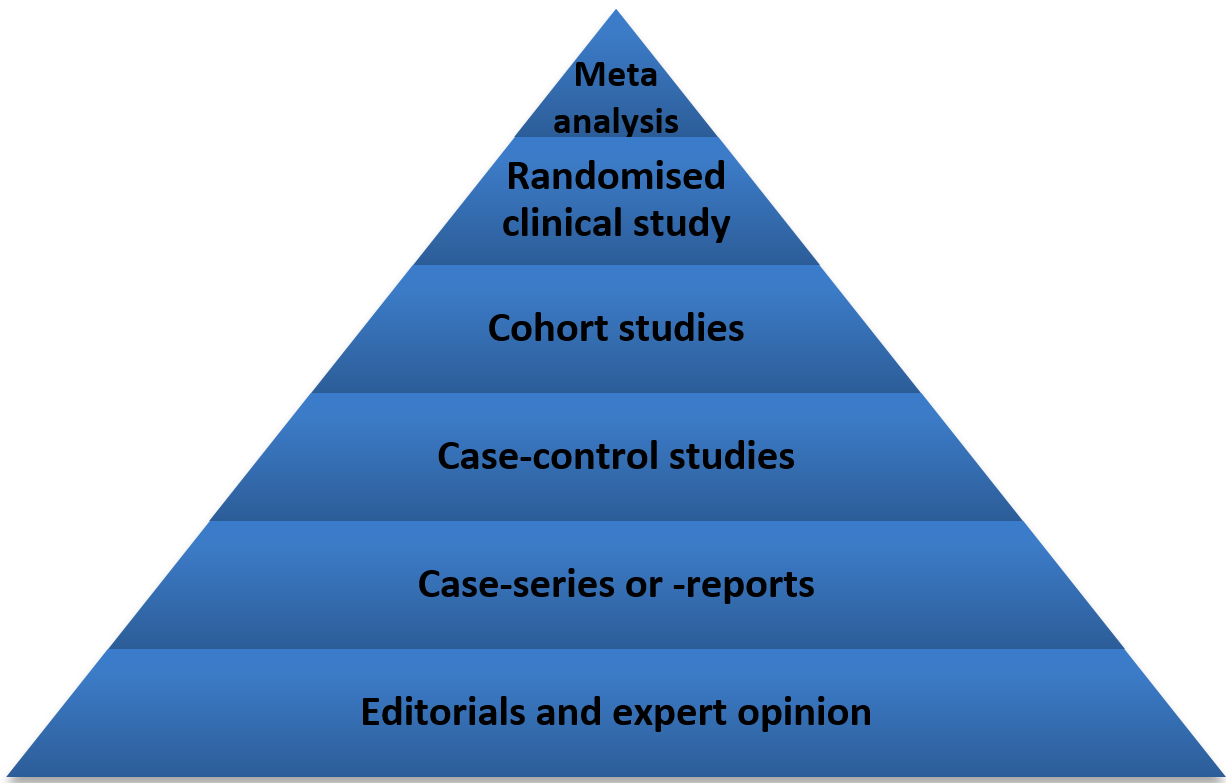
Figure 1. Various levels of evidence and their rankings; meta-analysis having the highest level of evidence and editorials and expert opinions the lowest.
-
-
Clinical outcome research seeks to monitor, understand and improve the impact of medical treatment on a specific patient or population. It does this by focusing on the clinical endpoints (overall outcomes). Some of these endpoints are reported directly by the patients. They could be quality of life or pain level. The main focus of outcome research is clinically relevant endpoints which means that they are directly related to the treatment of interest.Consider a clinical study where the effect of penicillin treatment is measured by the decrease of the amount of a specific protein (called ‘C-reactive protein’), always present in the blood. In a healthy person, the amount of this protein in the blood is very small, but it increases dramatically upon acute infection. This is therefore an indirect method to measure infection in the body. In this case the protein measured would serve as a ‘biomarker’ for an infection. A biomarker is a measurable indicator of a disease state. More specifically, a biomarker indicates a change in the amount or state of a protein. This then correlates with the risk or progress of a disease, or with how the disease is likely to respond to a given treatment. In daily practice, a blood sample is taken from the patient and the amount of the specific plasma protein measured.
For outcome research, the endpoint would not be the amount of the biomarker, but rather something felt or observed by the patient receiving the treatment. In the case of penicillin, the patient might be less concerned with the biomarker level, and instead be concerned with no longer having a fever and feeling better. This means that their symptoms and the way they feel would be considered a direct assessment of their health status. This is separate from the measure of a biomarker.
Many researchers define Patient Reported Outcomes as ‘relevant or important to patients’ however this is not always true. Patients and doctors may not always agree on which measures are important. What is clinically manageable may not necessarily be important to patients just because they are able to report on the specific measure. Therefore it is important to validate and document ‘patient relevance’ equal to what is clinically relevant when choosing Patient Reported Outcome measures.
Moreover, the patient is also likely to be interested in potential side effects associated with the penicillin as well as the cost of the treatment. Examples of endpoints are listed in Table 1.
ENDPOINT EXAMPLE Physiological measure - Blood pressure
Clinical - Heart failure
Symptoms - Coughing
Functional and care - Measurement of function (e.g. ability to perform tasks of everyday living; questionnaires about Quality of Life)
Table 1: Examples of endpoints relevant to outcome research studies.
For cancer, an important clinical outcome relevant for the patient is the risk of dying from cancer (for the researcher ‘survival rate’). Where there is a long study duration, outcome research studies can include the use of ‘surrogate endpoints’.
A surrogate endpoint is when a biomarker is used to measure an outcome – it acts as a substitute for a clinical efficacy endpoint.
Surrogate endpoints are a subset of pharmacodynamic biomarkers. These biomarkers are expected to predict clinical benefit (or harm, or lack of benefit or harm) based on epidemiologic, therapeutic, pathophysiologic, or other scientific evidence. Surrogate endpoints do not directly measure any clinical benefit to the patient, but predict benefit, such as a reduction in morbidity (incidence of a disease) or mortality (death).
Not all biomarkers are considered surrogate endpoints. For example, you might look at the presence of biomarkers related to cancer found in blood samples taken from the patient. If the level of the biomarker goes up, the cancer gets worse and if it goes down the cancer gets better. In the context of a clinical trial, surrogates are selected because they are more readily observed, are less invasive, and/or are apparent sooner or more frequently that the ultimate outcome measure. Biomarkers that relate to significant changes in disease state, as described above, do not meet these criteria.
It has to be underlined that for a surrogate endpoint to be used for regulatory purposes, the marker should have previously been confirmed or validated. It must be shown that changes in the biomarker correlate (correspond) with the clinical outcome of a specific disease and the treatment effect.
-
The most powerful tool to develop guidelines for the recommendation of evidence based medicines is the Grading of Recommendation Assessment, Development and Evaluation (GRADE) system. It is not used by all existing guidelines (which are often based on ‘expert opinions’), but it is the most stringent system assuring that the therapeutic recommendations are really based on evidence. It is the only system that the World Health Organisation (WHO) uses for its recommendations.
The GRADE system drives the experts who are designing new guidelines, through a pathway which starts from the review of the quality of the available evidence (which may be high, moderate, low and very low) and arrives at a certain recommendation (which may be strong or weak/conditional).
Figures 3 and 4 below show the different aspects taken into consideration by the GRADE system to evaluate the quality of the evidence and influence the final recommendation(s).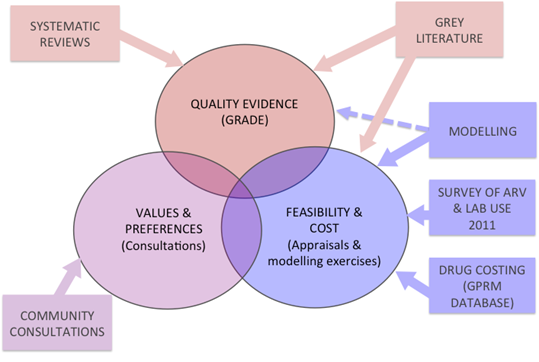
Figure 3: Aspects taken into consideration by the GRADE system.
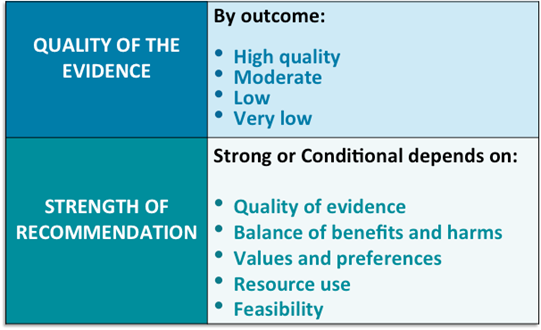
Figure 4: Grade quality of the evidence and strength of the recommendation.
-
-
Learners mustReceive a gradeReceive a passing grade
To receive a certificate for this course, you must be enrolled in the course (click on 'Enrol me in this course' yellow button at the top right on the course page), then complete the assessment and obtain at least 70% of correct answers. You have 10 attempts in total. Good luck!
-
Concepts of Evidence-Based Medicines and Outcomes Research
After completing this course, you will be able to:
- Outline the concepts of evidence-based medicine and outcomes research.