5. Patient involvement in different phases of HTA - Assessment
| Site: | EUPATI Open Classroom |
| Course: | Patient Involvement in HTA |
| Book: | 5. Patient involvement in different phases of HTA - Assessment |
| Printed by: | Guest user |
| Date: | Wednesday, 24 June 2026, 11:18 AM |
Description
1. Patient involvement in different phases of HTA
The figure below illustrates a simplified HTA process, highlighting where patients play a prominent role (solid lines) and where their involvement is more limited (dotted lines).
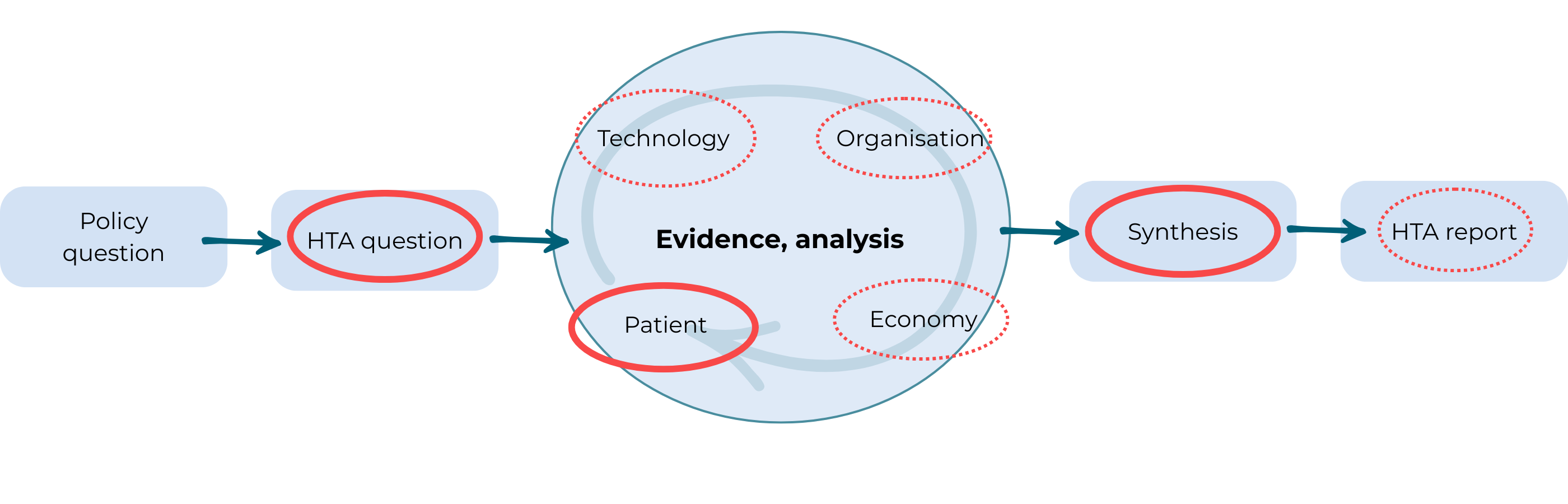
Figure 1 HTA process and patients’ role
In recent years, several HTA bodies have formally recognised patient perspective as one out of four pillars that should be evaluated:
- Clinical Effect and Safety
- Patient Perspective
- Health Care Organisation
- Economy
Acknowledging the patient perspective is increasingly seen as both an ethical obligation and a democratic imperative. While this does not necessarily simplify the HTA process, it reflects growing recognition among policymakers and HTA agencies of the importance of understanding patients’ experiences, needs, and preferences.
As patient organisations become more experienced in the HTA domain, they are playing a stronger role in shaping policy discussions and access-related debates. Their contributions are influencing HTA recommendations, supporting advocacy for new therapies, and improving the appropriate use of existing treatments.
Patients can meaningfully contribute to a wide range of HTA activities, including
ℹ️ Click on the Information buttons on the figure below to learn more about the three key phases
Forming the HTA questions: Policy and HTA
The formulation of HTA questions is a critical step, particularly for patients, as it influences the choice of methods, assessment process, and synthesis of findings. It is therefore essential that patients are included at this stage. The formulation of HTA questions occurs within the context of the anticipated decision-making scenario and is shaped by the knowledge of decision-makers, the target group, and relevant stakeholders. Including patients among the stakeholders who help formulate the HTA questions ensures that aspects important to them are adequately reflected in the assessment.
If patients are not involved at this stage, they can advocate for greater transparency, request opportunities to contribute through public consultation, or seek direct engagement prior to the formulation of the HTA questions.
HTA bodies must assess the added value of a new health technology using the best available information. This data may include clinical research as well as patient-reported experiences. Such assessments can involve qualitative and/or quantitative research approaches, which are further explored in:
- Course: HTA and Evaluation Methods: Quantitative | EUPATI Open Classroom
- Course: HTA and Evaluation Methods: Qualitative | EUPATI Open Classroom
It is also important to review research questions from previous HTA reports and literature, while avoiding the uncritical reuse of data. Each HTA must reflect the specific context—such as target group, disease stage, or healthcare setting. Patients can play a key role in evaluating whether existing data is applicable or whether new evidence is needed for the current situation.
Exploration of patient aspects
Health Technology Assessments (HTAs) have traditionally been developed based on expert knowledge of a given health technology, primarily to support political and administrative decision-making. A review of 50 HTA reports from eight countries covering the period 2000–2005 revealed that clinical studies are typically used as the main source when discussing patient aspects—rather than the actual effects experienced by patients in their daily lives or treatment situations (10). This is despite the fact that only the patient has direct experience of the full course of events.
In recent years, the importance of incorporating patients’ own experiences, preferences, resources, needs, and assessments into HTAs has grown. Including local patients in various roles helps ensure that the data and evidence assessed reflect national and local patient realities.
Individual Perspective
Focuses on the individual patient’s experiences in relation to everyday life.
Group Perspective
Captures collective experiences and assessments from a group of patients regarding how a given technology affects their daily lives.
Social Perspective
Considers patients as citizens, users, and consumers, including their views on how technologies should be prioritized and what criteria should guide their adoption.
This multi-perspective approach ensures inclusion of the following in the evidence assessment:
- 💡 Patients’ knowledge and lived experiences with the technology
- 🎯 Preferences, needs, and expectations regarding the technology
- 🔧 Patients’ visions and requirements for how the technology should function or be implemented
- 💼 Economic and organisational aspects (impact on the individual patient)
- 🌍 Influence of customs, attitudes, and traditions on patient’s experiences and preferences
- ❤️ What importance the technology has or may have for the patient’s everyday life
- 📈 The technology’s relevance and impact on patient’s everyday life
- 🤝 Ways to better support patient self-care and enhance empowerment resources
- ⚖️ Opportunities and limitations related to self-care and empowerment
To ensure HTAs are high-quality and transparent—and that decision-makers have a well-founded basis for their choices—evidence relating to the above aspects must be gathered and presented scientifically. Accordingly, patients and organizations should ensure that their representatives on boards, committees, and working groups possess a sound understanding of how to produce, interpret, and apply such data.
The following sections provide recommendations on when and how patients can contribute to the HTA process by helping define, interpret, and synthesize the data that is most meaningful and relevant to them.
Patient input in HTA's
Patients’ knowledge, experiences, and attitudes toward illness, suffering, treatment, and health technologies are deeply rooted in everyday life. These perspectives are shaped by personal experiences, those of close others, and a shared everyday culture.
Historically, international HTA reports often regarded the “patient” as part of the health technology being assessed [6]. However, in recent years, there has been a shift towards addressing patient aspects as a distinct focus. When examining these aspects, it is often useful to consider them separately from those related to the technology itself, organisational factors, or economic considerations. This can involve data from patient satisfaction surveys, studies on patient preferences, and qualitative research on patient needs, desires, and experiences.
Exploration of patient aspects in HTA
The model illustrates that various patient aspects are interrelated, though analytical clarity requires distinguishing them. Examples of areas for investigation include [7]:
ℹ️ Click on the Information buttons on the figure below to learn more about the different aspects
Patients can help identify which relationships between these aspects are most relevant, depending on the specific national or local context in which the HTA operates. While valid evidence may be available, it may not always reflect individual lived realities. Therefore, a careful evaluation of the social, ethical, and political context is essential. Patients should critically assess the applicability of the evidence included in the HTA.
Providing evidence on patient aspects
There are numerous ways in which patients can contribute to HTA discussions and ensure the inclusion of evidence on patient-relevant outcomes and the impact of treatments on daily life.
Patients can help identify appropriate research methods for eliciting, collecting, and evaluating patient outcomes, experiences, and preferences. Since patient perspectives may vary widely, using unsystematic or non-standardized approaches risks producing assessments that do not adequately reflect broader patient views. Patients can play a key role in developing, validating, and evaluating tools and methodologies that ensure reliable data collection and interpretation.
To ensure patient perspectives are meaningfully included, it is essential that participating patients understand the connection between qualitative insights (what is at stake, why it matters, and the implications) and quantitative data (how many, how much, for how long). They should also be able to support the translation of qualitative findings into measurable outcomes and contribute to comparisons or preference evaluations.
Patients may support the integration of patient-relevant outcomes, health-related quality of life (HRQoL), and preference measures in several ways:
Developing and/or validating patient-reported outcome measures (PROMs): This helps regulators, HTA bodies, and pharmaceutical companies determine which concepts and domains should be measured during clinical trials to generate credible HRQoL results.
Evaluating PRO/HRQoL measures and claimed changes: Patients can assess the relevance of the concepts, domains, and magnitude of changes used in HTAs, especially when PROMs from clinical trials do not fully reflect patients' views.
Endorsing specific PRO/HRQoL instruments: This applies both to clinical trials and other research efforts such as surveys.
Supporting the development, validation, or evaluation of patient preference measures: This includes helping identify relevant technologies and attributes for comparison.
Sharing patient experiences with HTA bodies: These narratives can highlight burdens not always captured in trial data, such as challenges with polypharmacy, which can inform whether a new medicine reduces such burdens.
Providing structured patient-group submissions: These submissions should enable HTA bodies to assess impacts across various decision criteria compared to current alternatives (e.g., equity, ethical, legal, psycho-social) in a balanced, comprehensive, and representative way.