1. Case-control studies
1.2. Case-Control Studies: Points to consider
Retrospective cohort studies are NOT the same as case-control studies: Cohort studies start out by classifying a group of people according to an exposure. Then, the investigator determines whether the exposed and unexposed people develop a disease or not. Case-control studies first identify a group of people with a disease. Then the investigator selects a comparison or control group without the disease. The two groups are compared and analysed for exposures. Because case-control studies begin with people who are sick or not sick, and examine previous exposures, they are retrospective.
Advantages
- can examine rare outcomes or outcomes with long latency because subjects are selected from the outset by their outcome status and the analysis is retrospective
- relatively quick to conduct
- relatively inexpensive to perform
- require comparatively few subjects
- existing records can be used
- multiple exposures or risk factors can be examined for one outcome, enabling a better understanding of possible risk factors for the outcome / disease
- no ethical issues in terms of collecting data if legally accessible
- many aetiological factors can be observed at the same time
- no need for follow up
Drawbacks
- particularly prone to recall bias
- difficult to validate information
- control of extraneous variables difficult and may be incomplete
selection of an appropriate comparison group cumbersome
- can only assess one
outcome within one analysis
- cannot establish prevalence
- quality of historic data often insufficient
Example: A paediatrician wants to study the association between the use of tap water for drinking and diarrhoea. His hypothesis is that “children using tap water for drinking are more likely to suffer from diarrhoea as compared to those who use mineral water”. In this example children who are suffering from diarrhoea will be cases while those not having diarrhoea will be controls. The exposure in this study is the use of tap water for drinking while the outcome is diarrhoea. Cases and controls are questioned, or their medical records are consulted regarding past exposure to risk factors (in this example tap water).
Later measure of association is determined which in a case-control study is “Odd Ratio” (K Park, 20th edition).
Example: Another case-control study design is by Chung[1] and colleagues, who examined maternal cigarette smoking during pregnancy and the risk of new-borns developing cleft lip/palate. A salient feature of this study is the use of the 1996 U.S. Natality database, a population database, from which both cases and controls were selected. This database provides a large sample size to assess new-born development of cleft lip/palate (outcome), which has a reported incidence of 1 in 1000 live births, and also enabled the investigators to choose controls (i.e., healthy new-borns) that were generalizable to the general population to strengthen the study's external validity. A significant relationship with maternal cigarette smoking and cleft lip/palate in the new-born was reported in this study (adjusted Odds ratio (OR) 1.34, 95% Confidence Interval (CI) 1.36-1.76). You can find more information about Odds ration in Statistics course.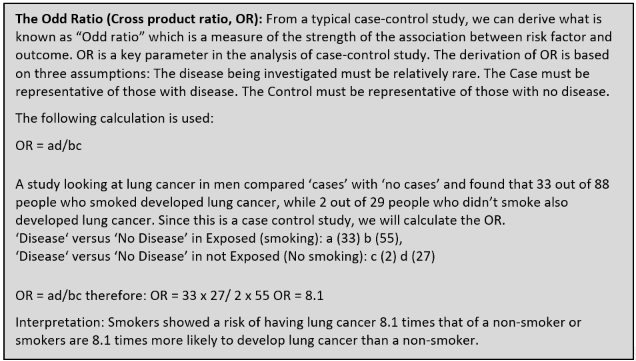
[1] Chung KC, Kowalski CP,
Kim HM, Buchman SR. Maternal cigarette smoking during pregnancy and the risk of having a
child with cleft lip/palate. Plast Reconstr Surg. 2000 Feb;105(2):485-91. doi:
10.1097/00006534-200002000-00001. PMID: 10697150.
https://pubmed.ncbi.nlm.nih.gov/10697150/